
Eyelid Laxity
Treatment of lax or loose eyelids — ectropion, entropion, floppy eyelid syndrome — causing discomfort, tearing, or corneal exposure.
Medically reviewed by Mark S. Brown, MD — ASOPRS fellowship-trained oculoplastic surgeon
Eyelid Laxity

Eyelid laxity describes loosening or weakening of the structural components that maintain the eyelids in their correct position against the globe. The most critical structures are the canthal tendons — the medial and lateral fibrous anchors that attach the eyelids to the bony orbital rim — along with the tarsal plate and the lower eyelid retractors. As these structures gradually lose tension with age, the lower eyelid may turn outward (ectropion), inward (entropion), or sag away from the eye in a way that disrupts normal tear drainage and corneal protection.
Common Symptoms
- Excessive tearing — when the punctum separates from the tear lake, tears overflow onto the cheek instead of draining normally
- Eye redness, irritation, burning, and foreign-body sensation
- Eyelashes rubbing against the cornea (trichiasis)
- Corneal exposure from incomplete eyelid closure
- Mucous discharge and crusting, particularly on waking
- Sensitivity to light and wind
Surgical correction is tailored to the specific type of malposition and the patient’s anatomy. An oculoplastic surgeon evaluates canthal tendon laxity, retractor integrity, and lamellar balance to determine the most appropriate repair.
For a detailed guide to eyelid anatomy, see our dedicated Eyelid Anatomy page.
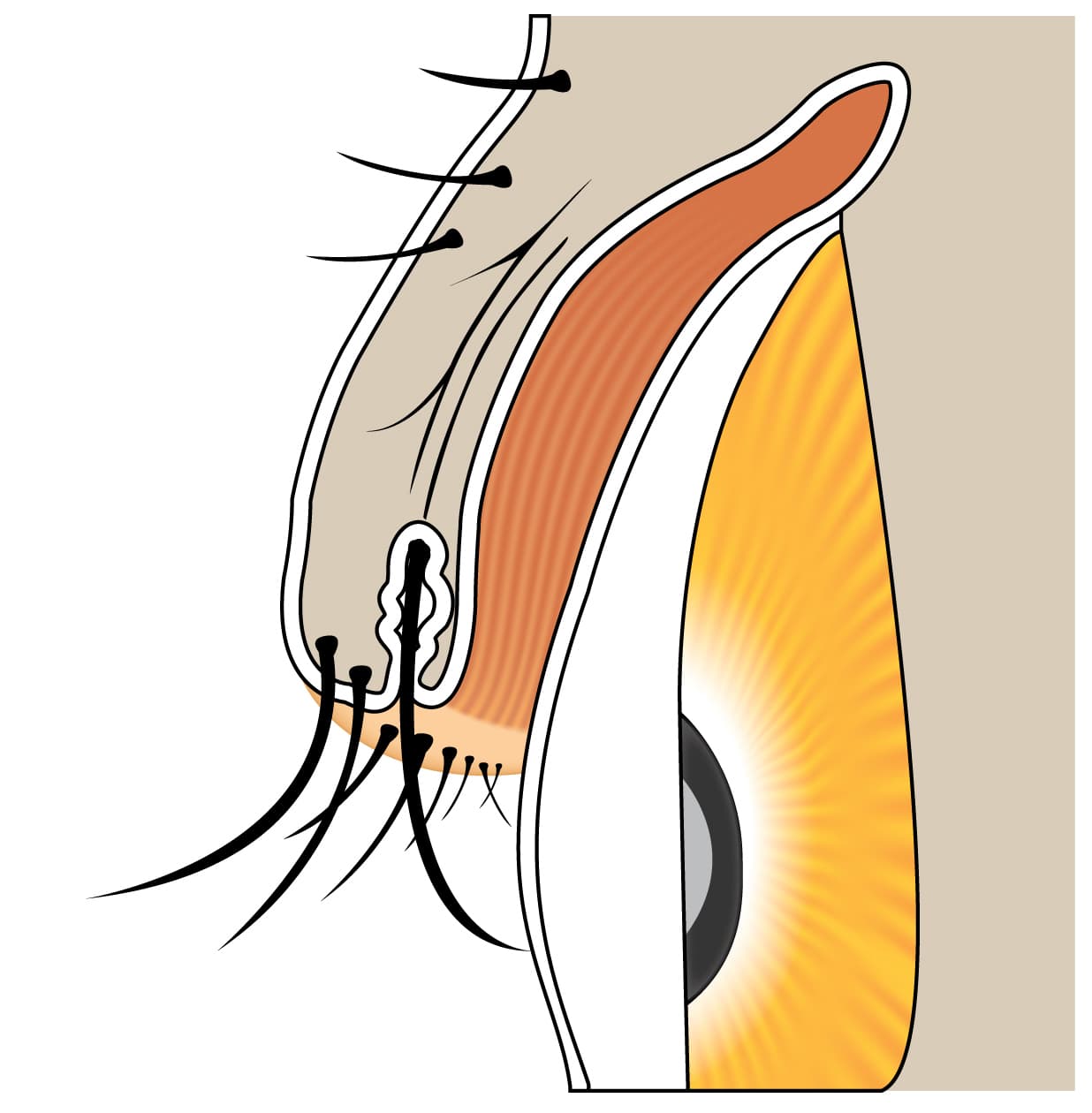
Ectropion

Ectropion is the outward turning of the lower eyelid margin away from the eye. When the lid no longer contacts the globe, tears cannot drain normally and the exposed conjunctiva becomes chronically irritated and inflamed.
Symptoms
- Excessive tearing and watery eyes
- Eye redness, irritation, and burning sensation
- Mucous discharge and eyelid crusting, especially in the morning
- Sensitivity to light and wind
- Risk of corneal damage from chronic exposure if untreated
Types of Ectropion
- Involutional (age-related) — the most common type, caused by gradual relaxation and horizontal laxity of the canthal tendons and supporting tissue. Treated with lateral canthoplasty or a tarsal strip procedure to re-anchor the lateral canthal tendon.
- Cicatricial — caused by scarring of the outer eyelid skin from burns, trauma, skin cancer, radiation, or chronic inflammatory skin conditions such as rosacea, eczema, or herpes zoster. Treatment restores vertical lid height, often with a full-thickness skin graft.
- Paralytic — caused by weakness of the orbicularis muscle from facial nerve (CN VII) palsy due to Bell’s palsy, acoustic neuroma, or parotid or temporal bone tumors. Options include lubricating drops, a gold weight implant to aid eyelid closure, lower lid sling, or lateral tarsorrhaphy.
- Mechanical — a mass or growth physically pulling the eyelid away from the globe; excision of the lesion is the primary treatment.
- Punctal ectropion — outward displacement limited to the tear drainage opening (punctum), causing chronic tearing even when the overall lid position appears normal. Addressed with a minor punctoplasty procedure.
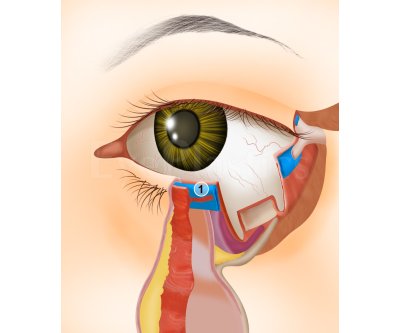
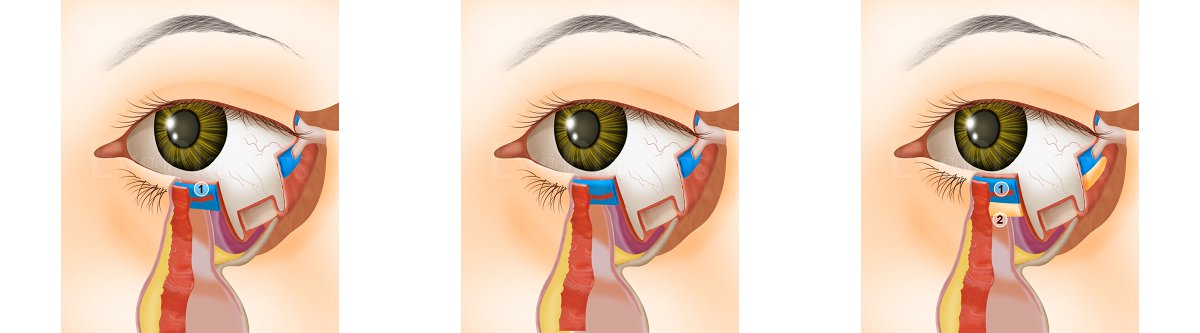
Surgical Treatments
Interactive animation covering lower eyelid retraction anatomy and both the External and Internal surgical correction approaches.
Lower Eyelid Retraction Correction — Surgical Animation
Entropion

Entropion is the inward turning of the eyelid margin, causing eyelashes to rub against the cornea and conjunctiva. This chronic friction produces persistent irritation, tearing, redness, and — if left untreated — corneal scarring and vision loss.
Four Anatomic Factors That Cause Involutional Entropion
- Horizontal lid laxity from canthal tendon stretching
- Lower eyelid retractor dehiscence (detachment or weakening)
- Preseptal orbicularis override rolling the lid margin inward
- Enophthalmos (sunken globe reducing posterior support)
Types of Entropion
- Involutional (age-related) — the most common form. Corrected surgically by addressing all contributing anatomic factors: retractor re-attachment, tarsal strip, and orbicularis repositioning.
- Cicatricial — caused by scarring of the inner eyelid surface from trachoma, Stevens-Johnson syndrome, chemical burns, ocular cicatricial pemphigoid, or prior surgery. Treated with mucous membrane grafting, lamellar rotation, or scleral grafts.
- Acute spastic — triggered by ocular inflammation or irritation. Often resolves when the underlying cause is treated; Quickert sutures provide temporary relief pending definitive repair.
- Congenital — rare; must be distinguished from epiblepharon, a common Asian pediatric condition. Treated by excising a small strip of skin and orbicularis below the lid margin.
Treatment Options
- Quickert sutures (temporary, office procedure)
- Thermal cautery (temporary)
- Lower eyelid retractor re-attachment
- Horizontal lid shortening (tarsal strip procedure)
- Full-thickness lid-splitting and marginal rotation
- Mucous membrane graft (cicatricial cases)
Floppy Eyelid Syndrome

Floppy eyelid syndrome (FES) is an uncommon condition in which the upper eyelid is unusually lax and rubbery, everting (turning inside out) with minimal pressure — or spontaneously during sleep when the face contacts a pillow. Nocturnal eversion causes the tarsal conjunctiva to rub against the bedding, producing chronic ocular surface inflammation.
Who Is Affected
FES is most common in overweight, middle-aged men. There is a striking association with obstructive sleep apnea (OSA), found in up to 96% of FES patients, making evaluation for OSA an essential part of management.
Pathophysiology
Histopathologic studies demonstrate a marked reduction in tarsal elastin, causing the tarsal plate to lose its normal rigidity and become rubbery and easily deformable. Some patients may have an underlying genetic predisposition to collagen or elastin abnormalities.
Clinical Findings
- Chronic papillary (“cobblestone”) conjunctivitis, often worse on the habitual sleeping side
- Mucous discharge and foreign-body sensation, particularly on waking
- Punctate corneal erosions from nocturnal mechanical rubbing
- Upper lid eversion with minimal manipulation; distinctly “rubbery” or doughy feel to the tarsus
- Associated conditions: keratoconus, meibomian gland dysfunction, blepharitis, seasonal allergic conjunctivitis
Management
Lubrication: preservative-free artificial tears during the day and lubricating ointment at bedtime protect the corneal surface.
Physical barriers: an eye shield or tape applied before sleep prevents spontaneous lid eversion and reduces nocturnal corneal trauma.
Surgical tightening: horizontal lid-shortening procedures (lateral canthoplasty or full-thickness resection) restore adequate tarsal tension in cases that do not respond to conservative management. Lateral tarsorrhaphy is reserved for severe or noncompliant patients.
OSA management: CPAP therapy and weight loss are strongly recommended alongside eyelid treatment. Adequate OSA therapy has been shown to produce notable improvement in FES. OSA also carries serious cardiovascular risks — including pulmonary hypertension, congestive heart failure, and cardiac arrhythmia — that require independent attention.
Trichiasis
Trichiasis describes misdirected eyelashes that grow toward the eye instead of away from it. Unlike entropion, the eyelid margin itself is in a normal position, but individual lash follicles are aberrantly oriented, causing persistent foreign-body sensation and potential corneal scarring. Distichiasis is a related condition in which a second, aberrant row of lashes grows from the meibomian gland openings along the posterior lid margin.
Full guide: Trichiasis & Distichiasis — diagrams, photos, and all treatment options →

Causes
- Chronic blepharitis — the most common cause; repeated lid-margin inflammation gradually distorts follicle orientation over time
- Cicatricial conditions — trachoma, Stevens-Johnson syndrome, chemical burns, and ocular cicatricial pemphigoid scar the posterior lamella and redirect follicles
- Eyelid trauma or surgery — scarring from lacerations or prior eyelid procedures
- Herpes zoster ophthalmicus — dermatomal scarring can permanently redirect lash follicles
- Idiopathic — no identifiable cause in some patients
Treatment Options
- Epilation (manual lash removal) — simple and immediately effective, but temporary; lashes regrow in 4–6 weeks
- Electrolysis — electrical current destroys individual follicles; approximately 50–80% success rate per follicle per treatment
- Radiofrequency ablation — offers slightly higher precision than electrolysis for individual follicle destruction
- Cryotherapy — liquid nitrogen freezes multiple follicles simultaneously; effective for extensive trichiasis but may cause eyelid depigmentation and adjacent-tissue damage
- Argon laser ablation — selectively targets pigmented follicles; most effective for darkly pigmented lashes
- Surgical lid splitting and follicle excision — the most definitive option for extensive or recurrent trichiasis; performed under local anesthesia in an outpatient setting
Frequently Asked Questions
- What is ectropion?
- Ectropion is outward turning (eversion) of the lower eyelid, causing the inner eyelid surface to be exposed. It leads to tearing, redness, irritation, and corneal exposure. The most common cause is age-related laxity of the canthal tendons and lower eyelid retractors.
- What is entropion?
- Entropion is inward turning (inversion) of the eyelid, causing the eyelashes to rub against the cornea. It causes significant eye irritation, tearing, and can lead to corneal scarring if untreated. It is most commonly caused by age-related laxity of the lower eyelid retractors.
- How is ectropion or entropion repaired?
- Both are corrected surgically. Ectropion repair typically involves tightening the lower eyelid through a lateral canthopexy or canthoplasty. Entropion repair involves reinserting or tightening the lower eyelid retractors, often combined with horizontal lid tightening. Surgery is performed under local anesthesia in an outpatient setting.
- What is floppy eyelid syndrome?
- Floppy eyelid syndrome (FES) is a condition in which the upper eyelid is excessively lax and easily everts (flips inside out) during sleep, causing chronic papillary conjunctivitis and ocular surface irritation. It is associated with obesity and obstructive sleep apnea.
- What should I expect during a consultation for eyelid laxity treatment?
- During your consultation, your oculoplastic surgeon will examine your eyelids carefully, assess how loose or stretched they are, and determine how this is affecting your comfort and eye health. They will review your symptoms, discuss your medical history, and explain which treatment option is best suited for your specific condition. You'll have the opportunity to ask questions and understand what the procedure involves before making a decision.
- What happens after eyelid laxity surgery, and how long is recovery?
- Most patients experience mild swelling and bruising around the eyes for the first 1-2 weeks following surgery. You can typically return to light activities within a few days and resume normal exercise within 2-3 weeks, though complete healing may take several months. Your surgeon will provide specific post-operative instructions, including how to care for your incisions and when to schedule follow-up visits to monitor your healing.
- Am I a good candidate for eyelid laxity surgery?
- Good candidates are generally those experiencing symptoms from loose eyelids, such as excessive tearing, irritation, redness, or a feeling that the eyelid is drooping or rolling outward. Overall good health and realistic expectations about surgical outcomes are important factors. Your surgeon will evaluate your specific condition and medical history to determine if surgery is appropriate for you or if other treatments might be beneficial.
Find a Specialist
Connect with a board-certified oculoplastic surgeon who specializes in eyelid laxity.
Search the Directory →