Anophthalmos
Surgical and prosthetic management of anophthalmos (absence of the eye) and socket reconstruction following enucleation or evisceration.
Medically reviewed by EyePlastics Medical Editorial BoardASOPRS oculoplastic surgeonsLast updated June 2026
Anophthalmos — Overview
Anophthalmos (or anophthalmia) refers to the absence or loss of the eye within the orbit. The term covers a broad spectrum — from congenital absence of the globe, to acquired loss of the eye from trauma, tumor, or advanced ocular disease. Regardless of cause, the result is an empty or shrunken socket that requires reconstruction to restore volume, support a prosthesis, and maintain a natural facial appearance.
Modern orbital implants and socket-reconstruction techniques have transformed outcomes for patients with anophthalmos. ASOPRS-trained oculoplastic surgeons provide orbital implant surgery, socket reconstruction, and long-term prosthetic management for patients of all ages — including children with congenital conditions who need stimulation of orbital growth.
Classifications of Anophthalmos
Congenital anophthalmos is classified by the stage at which ocular development failed:
- Primary anophthalmia — complete absence of eye tissue from failure of the optic vesicle to develop as an outgrowth of the forebrain neuroectoderm.
- Secondary anophthalmia — the eye begins to develop but stops at an early stage, leaving only residual ocular tissue.
- Degenerative anophthalmia — a partially formed eye regresses, often from a disruption in blood supply during fetal development.
True primary anophthalmos is very rare; extreme microphthalmos (a very small globe within the orbital soft tissue) is more commonly encountered clinically. Anophthalmos and microphthalmos can occur as isolated findings or as part of syndromes associated with chromosomal abnormalities, including Trisomy 13.
Causes of Anophthalmos
Congenital anophthalmos may result from inherited or sporadic genetic mutations, chromosome abnormalities, prenatal environmental insults (infections, teratogens), or unknown causes. Development of the eyelids, conjunctival fornices, and bony orbit depends on the presence of a normal-sized eye during fetal growth; absence or severe reduction of the globe impairs orbital development and requires early intervention.
Acquired anophthalmos results from surgical removal of the eye for trauma (severe injury not amenable to repair), tumor (retinoblastoma, choroidal melanoma, other intraocular malignancies), infection (endophthalmitis unresponsive to treatment), or advanced ocular disease (end-stage glaucoma, a painful blind eye).

Surgical Options — Evisceration, Enucleation & Exenteration
When the eye cannot be saved, two primary procedures are available:
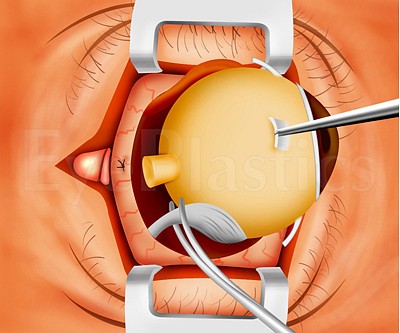
- Evisceration — removal of the intraocular contents while preserving the scleral shell. The sclera and extraocular muscles remain intact, which provides excellent implant motility. Evisceration is generally preferred when there is no concern for intraocular malignancy, as it preserves more tissue and often improves prosthetic movement. It carries a small theoretical risk of sympathetic ophthalmia, though this risk is rare and its comparison with enucleation remains debated.
- Enucleation — removal of the entire globe, including the sclera, leaving the extraocular muscles and orbital fat. Enucleation is required when intraocular malignancy is present or suspected. The extraocular muscles are then sutured to the orbital implant to restore movement.
- Exenteration — removal of the entire orbital contents (the eye, orbital fat and muscles, and sometimes the eyelids). It is the most radical option, reserved for life- or sight-threatening disease that has invaded the orbit — most often an aggressive orbital or eyelid malignancy, or an invasive infection such as mucormycosis. The resulting cavity is reconstructed with a skin graft or flap, or rehabilitated with an orbital (facial) prosthesis rather than a standard ocular prosthesis.
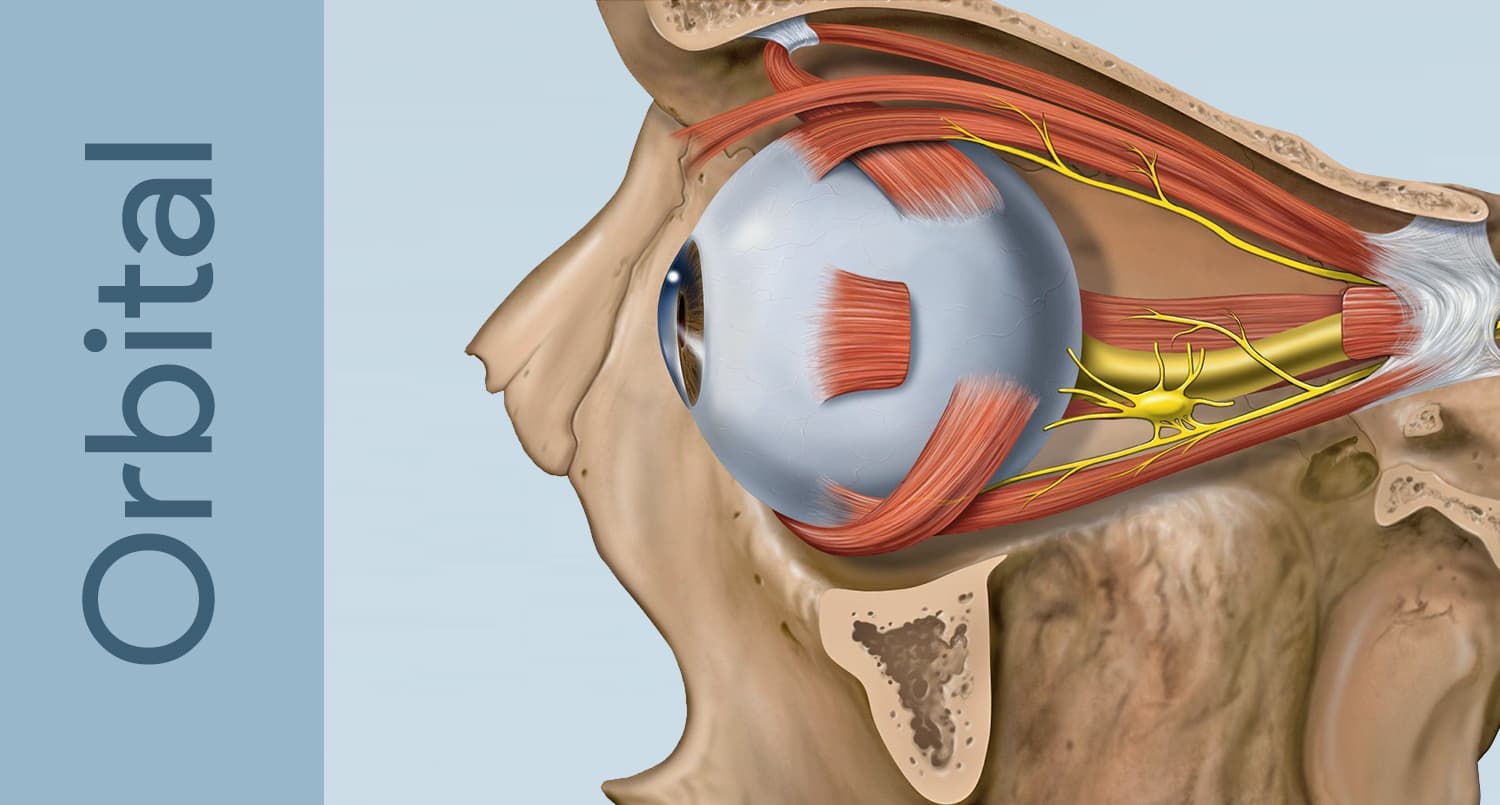
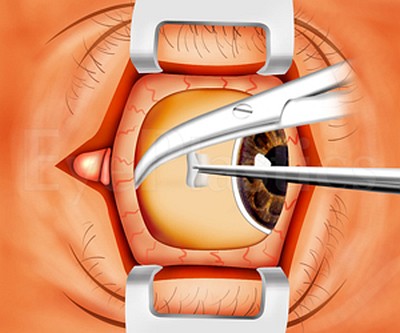
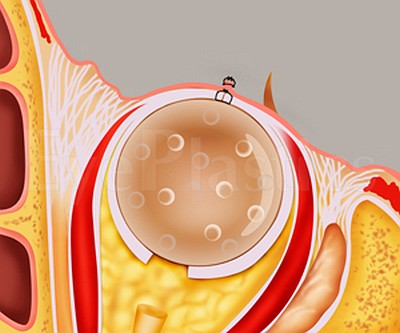
Following either procedure, an orbital implant is placed within the muscle cone to restore orbital volume, and a custom ocular prosthesis is fitted by an ocularist 4–6 weeks later. The animations below illustrate the relevant anatomy and both procedures step by step.
Anophthalmos SurgeryStep-by-Step
Choose a procedure, then drag the slider to step through it.
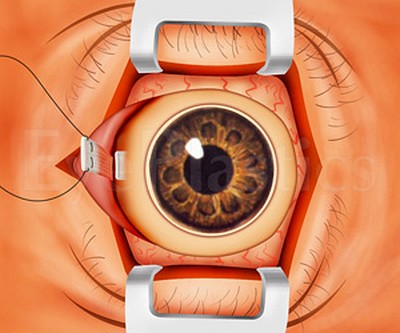
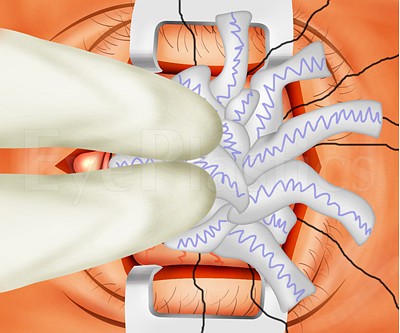

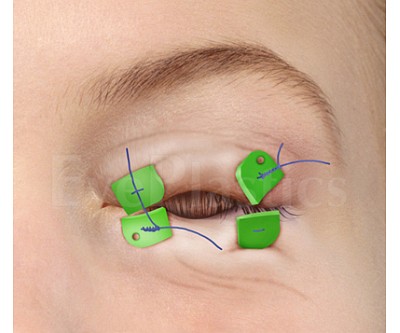

Step 1 of 16
The eye is exposed, ready for surgery
Drag the slider to compare
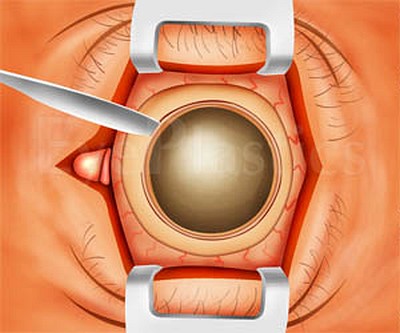
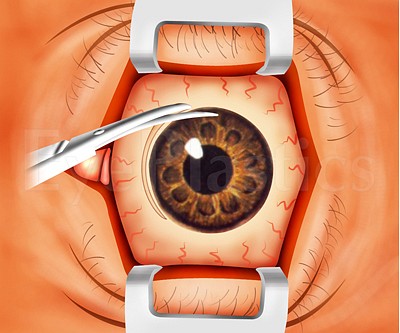
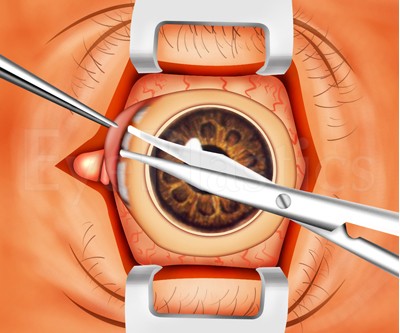
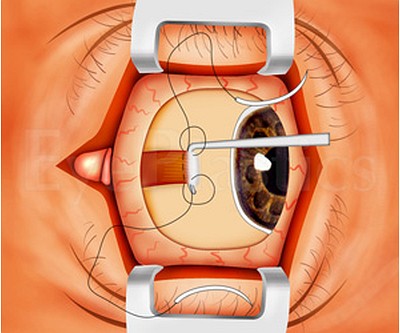
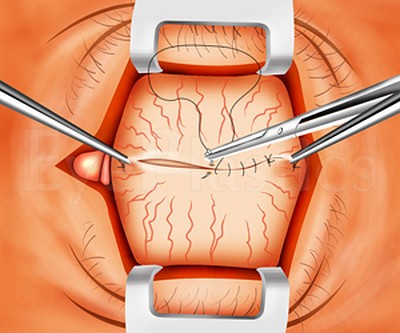
EviscerationActual Surgery Photographs
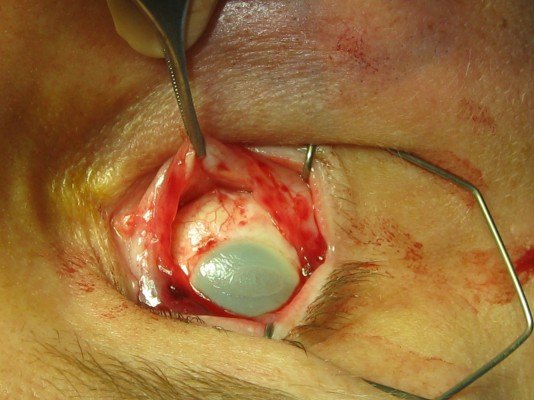
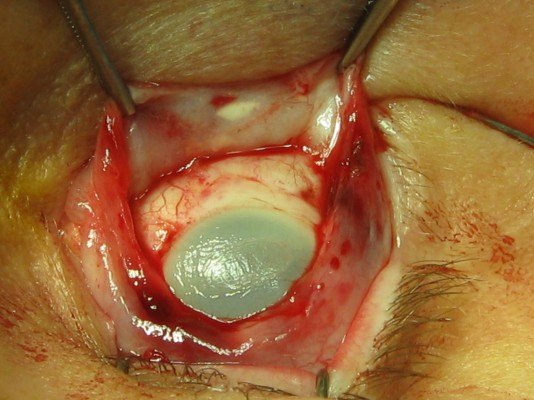
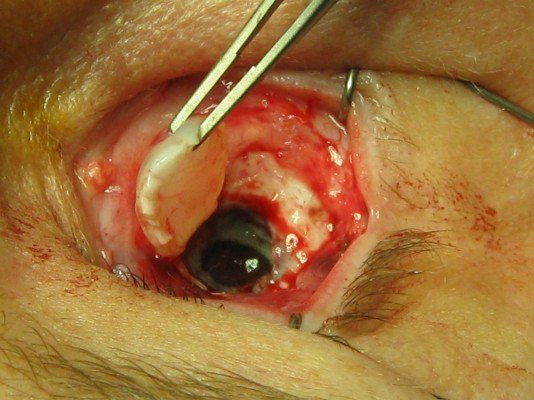
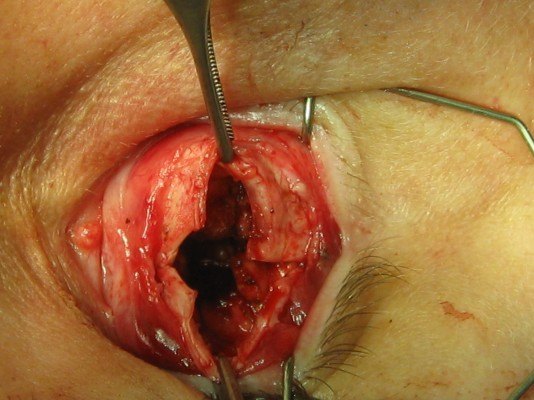
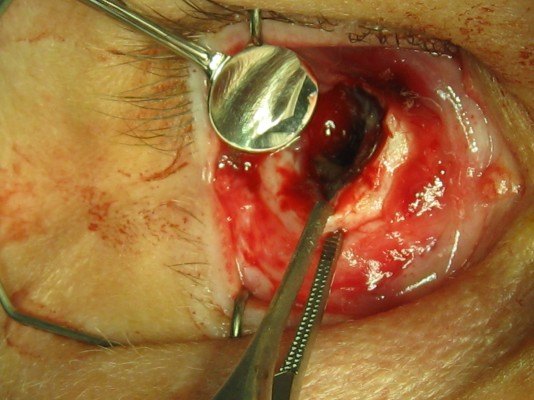
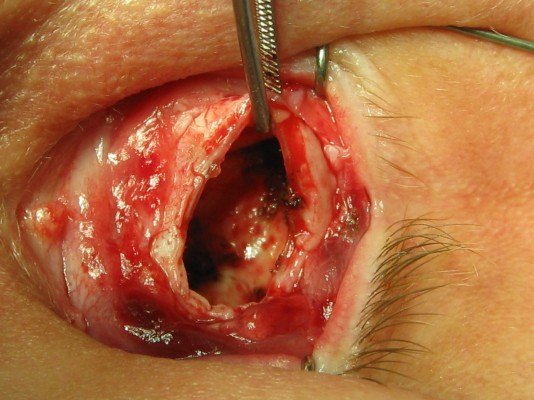
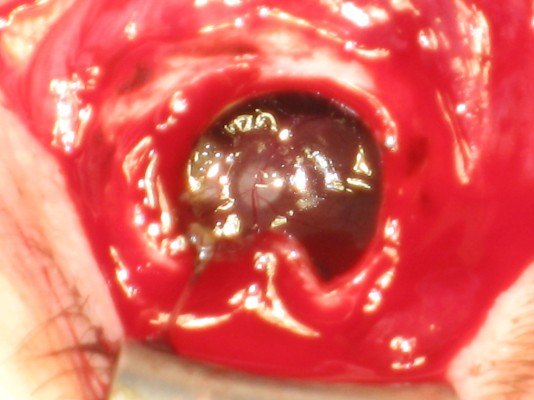
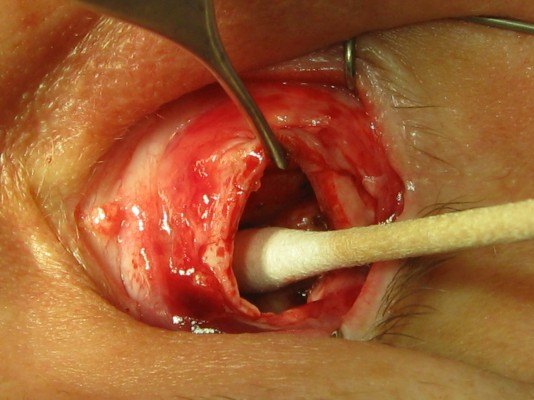
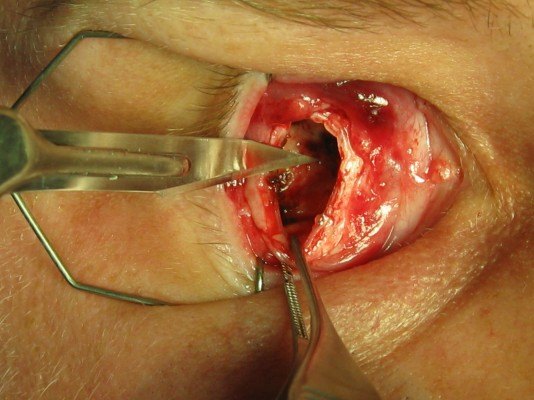
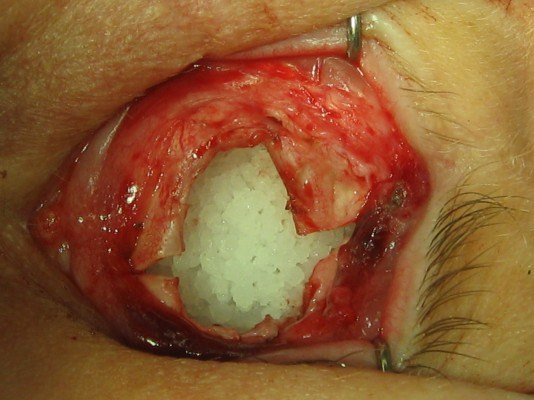
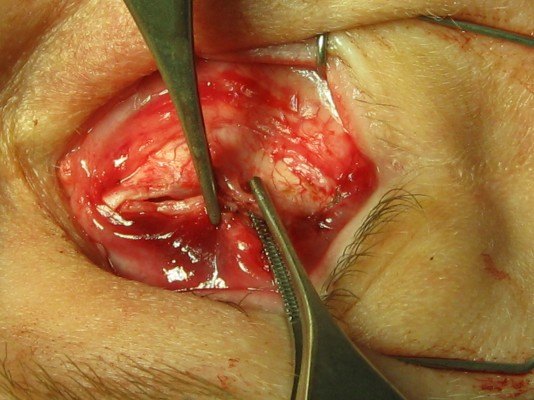




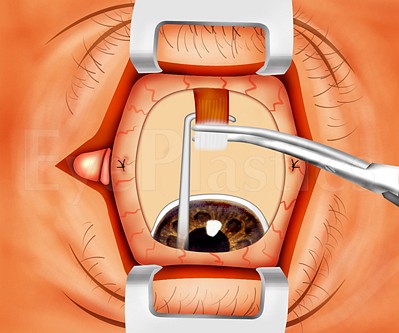
Step 1 of 15
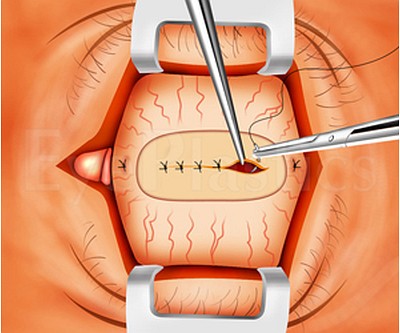
Opening the conjunctiva
Drag the slider to step through the evisceration technique. These are real surgical images.
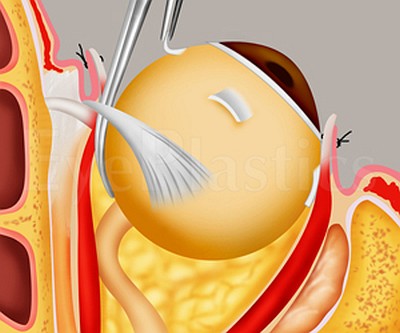
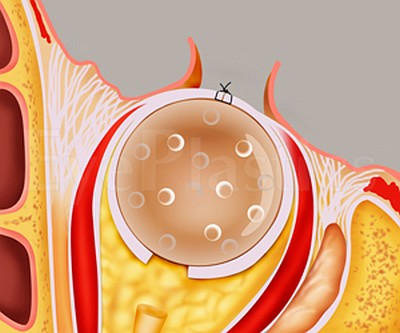
How orbital implants restore volume and movement after the eye is removed.
Retinoblastoma — Enucleation in Children
Retinoblastoma is the most common primary intraocular malignancy of childhood, arising from the developing retina and usually diagnosed before age five. It is one of the most important reasons an eye is removed in a child, and the oculoplastic and ocularist team plays a central role in reconstructing and maintaining the socket as the child grows.
Early sign — leukocoria. A white pupillary reflex (a white rather than red “red-eye” in flash photographs), a new eye turn (strabismus), or a red, painful eye in a young child should prompt urgent ophthalmology referral.
Genetics & presentation
- Caused by loss of both copies of the RB1 tumor-suppressor gene
- Heritable form (germline) is often bilateral/multifocal and carries a lifelong risk of second cancers; sporadic form is typically unilateral
- Presents with leukocoria, strabismus, or a red/inflamed eye; genetic counseling is recommended
Diagnosis & staging
- Dilated examination under anesthesia by an ocular oncologist
- B-scan ultrasound (shows calcification) and MRI of the orbits and brain
- Biopsy is avoided — entering the eye risks seeding tumor outside the globe
Eye-sparing treatment is the goal whenever the eye and useful vision can be saved — systemic or intra-arterial chemotherapy (chemoreduction), focal laser, cryotherapy, and plaque brachytherapy are used for less advanced tumors, ideally at a specialized ocular-oncology center.
When enucleation is indicated. Removal of the eye is recommended for advanced unilateral disease, when there is no prospect of useful vision, or when sparing the eye would risk spread of the tumor — particularly along the optic nerve. Two principles guide the surgery:
- Remove the globe intact with a long segment of optic nerve, without rupturing the eye, to reduce the risk of tumor seeding and to clear nerve involvement.
- Restore volume primarily — a porous orbital implant is placed at the time of enucleation, and an ocularist later fits a custom prosthesis, as described in the prosthesis and ocular implants sections.
Because the orbit is still growing, children with an anophthalmic socket need ongoing follow-up; a well-fitted, regularly upgraded prosthesis (and avoidance of unnecessary radiation when possible) helps the bony orbit and lids develop symmetrically. With early detection and modern treatment, survival in developed countries exceeds 95%, which is why recognizing leukocoria early is so important. Pathology and any need for additional chemotherapy or radiation are coordinated with pediatric oncology.
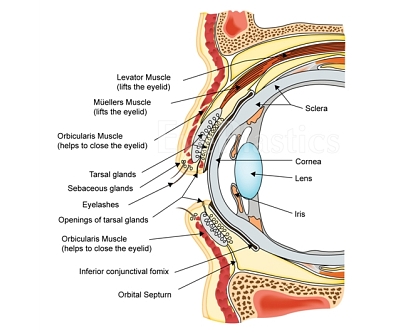
The Ocular Prosthesis
A custom ocular prosthesis (artificial eye) is fitted over the healed implant by a certified ocularist, who hand-paints it to match the fellow eye’s iris, limbus, and scleral vessels. The sequence below shows the progression from the healed socket to a fitted prosthesis.




Explore This Topic
- Ocular Implants & Scleral Shell — silicone/acrylic sphere, MEDPOR®, hydroxyapatite, bioceramic, and dermis-fat graft.
- Socket Complications — socket syndrome, exposure, and extrusion.
- Results & Motility — what well-fitted outcomes look like.
- Resources & References — support organizations and further reading.
Continue Reading — Complete Anophthalmos & Socket Guide
Frequently Asked Questions
- What is enucleation?
- Enucleation is surgical removal of the entire eyeball. It is performed for intraocular tumors (such as retinoblastoma or uveal melanoma), end-stage painful blind eyes, and severe trauma. An orbital implant (typically porous polyethylene or hydroxyapatite) is placed to restore volume, and a prosthetic eye (ocular prosthesis) is fitted over the implant.
- What is the difference between enucleation and evisceration?
- Evisceration removes only the internal contents of the eye while preserving the scleral shell and extraocular muscles, giving better prosthesis motility and often a faster recovery. Enucleation removes the entire globe. Evisceration is not appropriate when intraocular malignancy is suspected.
- How realistic does an ocular prosthesis look?
- Modern ocular prostheses, fitted by a certified ocularist, are highly realistic — custom-painted to match the fellow eye's iris, limbus, and scleral vessels. With proper fitting and regular polishing (every 1–2 years), most people cannot distinguish a well-fitted prosthesis from a natural eye in normal social interaction.
- What should I expect during my consultation for anophthalmos treatment?
- During your initial consultation, your oculoplastic surgeon will examine the eye socket, review your medical history, and discuss your goals for reconstruction and prosthetic fitting. They will explain the available surgical and prosthetic options, answer your questions, and help you understand the timeline and expected outcomes. Imaging studies may be ordered to assess socket dimensions and bone structure. This visit allows you and your surgeon to develop a personalized treatment plan suited to your specific needs.
- What happens after surgery to prepare for a prosthetic eye?
- After your socket reconstruction surgery heals—typically 4 to 6 weeks—your surgeon will assess socket volume, shape, and tissue integrity to ensure optimal conditions for prosthetic fitting. Once healing is complete, you'll be referred to an ocularist (a specialist trained in creating custom prosthetic eyes) who will take detailed measurements and impressions of your socket. The ocularist will fabricate a prosthesis customized to match your other eye in color, size, and appearance, with multiple fitting appointments to ensure comfort and proper alignment.
- What are the potential complications of socket reconstruction surgery?
- While socket reconstruction is generally safe, potential complications can include infection, bleeding, implant exposure, inadequate socket volume, and asymmetry compared to the opposite eye. Some patients may experience scarring that affects prosthetic fit or requires revision surgery. These risks are minimized when surgery is performed by an experienced oculoplastic surgeon using modern techniques and proper post-operative care. Your surgeon will discuss specific risks relevant to your situation during consultation.
- How do I care for my socket and prosthetic eye after treatment?
- Daily cleaning of your prosthetic eye with mild soap and water, along with regular socket hygiene, helps prevent infection and maintains comfort. Your prosthesis should be removed nightly to allow the socket to rest and be cleaned. Regular follow-up appointments with your oculoplastic surgeon ensure the socket remains healthy, and periodic visits to your ocularist allow for adjustments as the socket naturally changes shape over time. Proper care typically allows your prosthesis to function comfortably for many years.
Find a Specialist
Connect with a board-certified oculoplastic surgeon who specializes in anophthalmos.
Search the Directory →