Ptosis vs. Blepharoplasty: Which Eyelid Condition Do You Have?
The correct diagnosis determines the treatment — and whether insurance will cover it.
Ptosis — Drooping Eyelid Margin
The eyelid edge (margin) sits too low — partially covering the pupil. Caused by weakness or disinsertion of the levator muscle. The overlying skin may look completely normal.
Treatment: muscle surgery (ptosis repair)
Blepharoplasty — Excess Eyelid Skin
The eyelid margin is in its normal position, but excess skin (dermatochalasis) hangs over it — creating a heavy, tired appearance. The lifting muscle works normally.
Treatment: skin and fat removal
A Simple Self-Assessment
Stand in front of a mirror in good lighting. Look straight ahead — do not raise your brows.
1. When looking straight ahead — without raising your brows — does the upper eyelid cover part of your pupil?
If yes: this suggests ptosis. The eyelid margin itself sits too low.
2. Does excess skin hang over your upper eyelid, but the eyelid edge (near the lashes) appears to sit at a normal height?
If yes: this suggests dermatochalasis — you may be a blepharoplasty candidate.
3. Do you find yourself unconsciously raising your eyebrows throughout the day to see clearly, or tilting your chin up?
If yes: this compensation pattern occurs with both ptosis and excess skin — evaluation is needed.
4. Does the drooping worsen noticeably as the day progresses or after sustained reading?
If yes: fluctuating ptosis may indicate myasthenia gravis — a neurologic cause that must be excluded before any surgery.
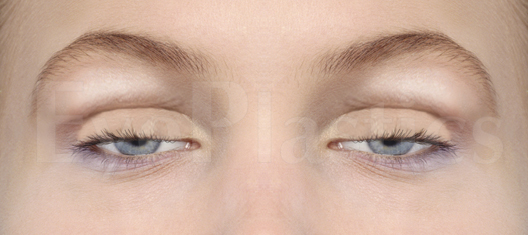
What Each Condition Looks Like

Ptosis — eyelid margin droops over the pupil

Dermatochalasis — excess skin hoods over normal lid margin
Side by Side: Ptosis vs. Dermatochalasis
The problem
Underlying cause
The skin
Other triggers
How it's corrected
What it does NOT fix
Insurance
How Ptosis Is Classified
Ptosis (blepharoptosis) is classified by origin (congenital or acquired), by cause (aponeurotic, myogenic, neurogenic, or mechanical), and — most importantly for surgical planning — by levator function: poor (≤ 4 mm), fair (5–9 mm), or good (≥ 10 mm). A ptotic eyelid covers more than 2 mm of the upper limbus; in severe cases it covers the pupil and obstructs vision, causing reading difficulty, headaches, and brow strain.
True ptosis must also be distinguished from pseudoptosis — an eyelid that only appears low because of excess skin, a small or displaced globe, or brow descent. It is particularly common in older patients after cataract or other intraocular surgery, where the levator is stretched by the eyelid retractor used during the operation.

Interactive: Ptosis Repair With vs. Without Blepharoplasty
Each surgical condition requires a distinct approach. Ptosis repair elevates the eyelid height (opens the eye wider), while blepharoplasty removes the excess skin and herniated fat. Drag the slider to see how the result differs when the two procedures are combined.











Drag the slider to compare how the eyelid changes when ptosis repair is performed alone versus combined with blepharoplasty.
When Both Are Present: The Combined Case
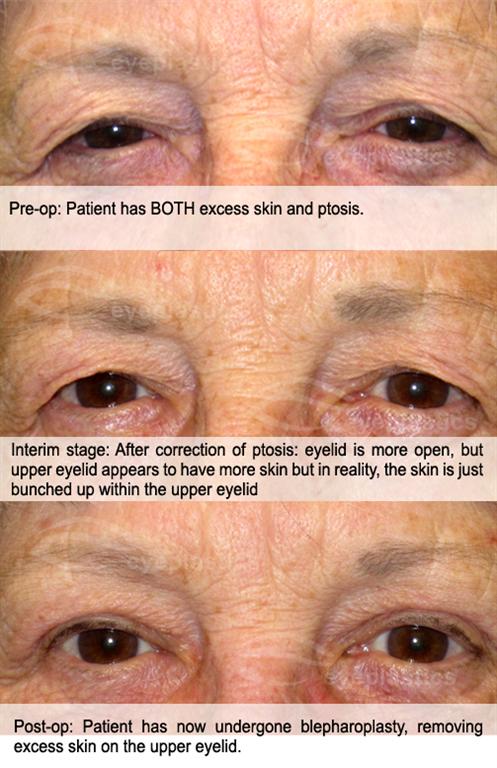
It is common — particularly in patients over 55 — to have both dermatochalasis and involutional ptosis simultaneously. Treating only one produces a suboptimal result:
- Blepharoplasty alone in a patient with unrecognized ptosis may “unmask” the drooping — removing the weight of excess skin reveals the margin is actually lower than expected
- Ptosis repair alone when significant dermatochalasis exists may leave the patient with persistent skin heaviness and incomplete improvement
When both conditions are identified preoperatively, your surgeon can address them in a single operative session, minimizing recovery time and anesthesia exposure.
Ptosis Repair with Blepharoplasty — Before & After
1 / 11In the cases below, note both changes of a combined repair: the lid margin rises off the pupil (the ptosis repair), and the skin hooding is gone even though the eyelid now sits higher — the blepharoplasty. Fixing only one would leave either a low lid or a heavy fold.
Drag the divider left or right to compare. Select a case in the strip below.


Find a Specialist
Connect with a board-certified oculoplastic surgeon who can evaluate both conditions and recommend the correct treatment in a single consultation.
Search the Directory →