Tepezza® — Teprotumumab Infusion
For Active Thyroid Eye Disease
Tepezza (teprotumumab-trbw) is the first FDA-approved medical therapy specifically targeting the underlying pathology of Thyroid Eye Disease. In clinical trials, it produced a ≥2 mm reduction in proptosis (bulging eyes) in 83% of patients — without surgery — and significantly improved double vision, lid retraction, and quality of life.
What Is Tepezza?
Tepezza (generic name: teprotumumab) is a fully human monoclonal antibody approved by the FDA in January 2020 for the treatment of active Thyroid Eye Disease (TED), also called Graves' ophthalmopathy. It is administered as an intravenous (IV) infusion in an outpatient infusion center or physician's office.
Before Tepezza, the only options for significant proptosis were IV steroids — which provided temporary relief — or surgical orbital decompression. Tepezza targets the disease mechanism directly, producing durable reductions in proptosis and inflammation that persist well beyond the completion of the treatment course.
ASOPRS fellowship-trained oculoplastic surgeons are uniquely qualified to manage Thyroid Eye Disease across its full natural history — from monitoring the active inflammatory phase and administering Tepezza, through surgical rehabilitation when the disease stabilizes.
How It Works
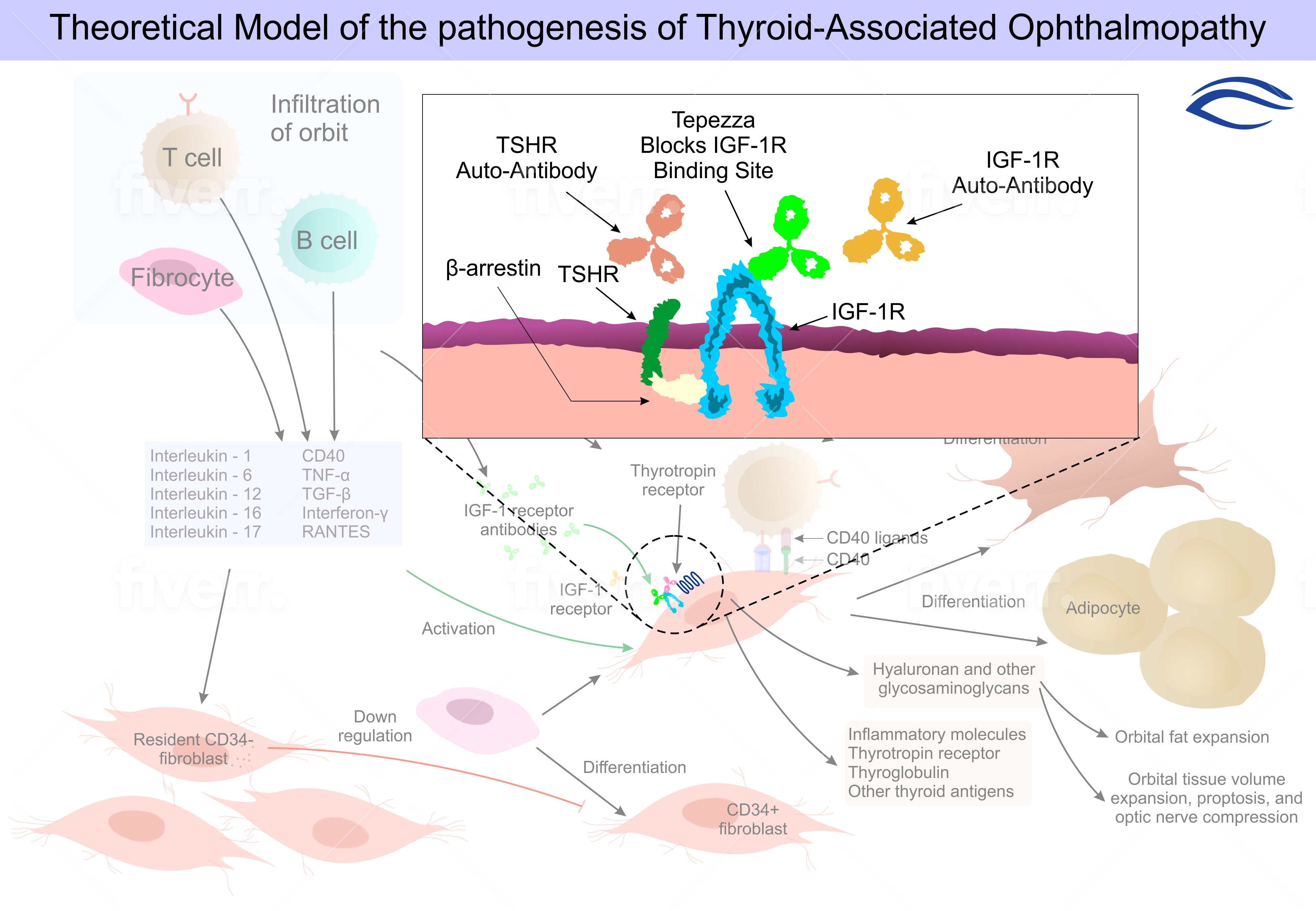
The hallmark of TED is activation of orbital fibroblasts — connective tissue cells within the orbit — by two key immune receptors: the thyroid-stimulating hormone receptor (TSHR) and the insulin-like growth factor-1 receptor (IGF-1R). When autoantibodies bind these receptors, fibroblasts proliferate, produce excess hyaluronic acid, and differentiate into fat cells, causing orbital volume to expand. The result is proptosis, lid retraction, double vision, and orbital pain.
Teprotumumab's Target: IGF-1R
Teprotumumab binds and blocks the IGF-1R receptor, interrupting the signal cascade that drives fibroblast activation. By silencing this pathway, the drug:
- Reduces hyaluronic acid production, decreasing orbital soft tissue volume
- Decreases proptosis — the forward protrusion of the eye
- Reduces orbital fat and extraocular muscle enlargement
- Improves lid retraction (upper and lower eyelid position)
- Reduces diplopia (double vision) from restrictive strabismus
- Decreases Clinical Activity Score (CAS) — the marker of active inflammation
Because teprotumumab acts on a different pathway than steroids, patients who have failed or cannot tolerate steroid therapy may still respond to Tepezza.
Clinical Trial Results
Tepezza was approved on the basis of two randomized, double-blind, placebo-controlled trials (OPTIC and its predecessor). Key results at week 24:
| Outcome | Tepezza | Placebo |
|---|---|---|
| Proptosis response (≥2 mm reduction) | 83% | 10% |
| Overall response rate | 78% | 7% |
| Mean proptosis reduction | 2.82 mm | 0.54 mm |
| Clinical Activity Score response | 59% | 21% |
| Diplopia response | 68% | 29% |
| Quality of life (GO-QOL) | +19.0 pts | +6.6 pts |
OPTIC Extension — Durability
In the OPTIC extension study, patients who responded to Tepezza maintained significant proptosis reductions at 51 weeks post-treatment, with most responders sustaining their improvements. Patients who relapsed after initial treatment responded well to a second course of teprotumumab.
Before & After
Tepezza characteristically reduces proptosis (eye bulging) and softens the inflammatory, staring appearance of active thyroid eye disease. Individual results vary.
Tepezza® Before & After
1 / 6Drag the divider left or right to compare. Select a case in the strip below.


Who Qualifies?
Tepezza is most effective in patients with active thyroid eye disease — meaning the inflammatory phase is ongoing. Key candidacy criteria:
✓Active inflammation
Clinical signs of active disease — a Clinical Activity Score (CAS) of at least 3 of 7 (pain with eye movement, redness, swelling, conjunctival injection). Tepezza works best during the active inflammatory phase; since the 2023 label update it is approved for TED regardless of activity score or duration, so candidacy is individualized.
✓Recent onset
Ideally within the first 9–12 months of symptom onset, when the inflammatory phase is most active and treatment response is highest.
✓Significant proptosis or diplopia
Proptosis ≥3 mm above normal, or new or worsening diplopia that impacts daily function.
✓Controlled thyroid function
Thyroid hormone levels should be stabilized with endocrinology management before or concurrent with Tepezza treatment.
Note on inactive TED: Patients in the inactive (quiescent) phase of TED — stable proptosis, no active inflammation — are not candidates for Tepezza and should be evaluated for surgical options including orbital decompression, strabismus surgery, and eyelid recession.
Treatment Protocol
Tepezza is administered as an IV infusion according to a standardized protocol:
10 mg/kg over 90 minutes. Baseline eye measurements, Clinical Activity Score, and blood glucose are recorded before starting.
20 mg/kg every 3 weeks. After the first one or two infusions are well tolerated, the infusion time may be shortened (to 60 and then 30 minutes). Total treatment: 24 weeks.
Eye exams and Hertel exophthalmometry at each visit track proptosis reduction. Blood glucose monitoring is recommended, especially in patients with diabetes or pre-diabetes.
Final measurements at week 24. Most patients reach maximum response by infusion 6–8. Stable disease can then be monitored; relapse is treated with a second course.
Side Effects & Monitoring
Most patients complete all 8 infusions, but Tepezza requires active monitoring — particularly of blood glucose and hearing — and the side effects below should be reviewed before starting treatment. The most clinically important to monitor:
Hyperglycemia (elevated blood glucose)
CommonBlood glucose can rise significantly during and after infusions. Patients with diabetes or pre-diabetes require close monitoring. All patients should have fasting glucose checked before each infusion.
Hearing changes (tinnitus, fullness, hearing loss)
Common — and potentially seriousHearing-related effects (tinnitus, ear fullness, autophony, hearing loss) were reported in about 10% of clinical-trial patients, but post-marketing studies using formal hearing testing found otologic symptoms in a majority of patients. Most symptoms (tinnitus, fullness, autophony) resolve after treatment, but some hearing loss can be permanent. The FDA label recommends audiologic assessment before, during, and after treatment — baseline and monitoring audiology is especially important for patients with pre-existing hearing problems.
Muscle cramps
Common (~25%)Usually mild and manageable with magnesium supplementation. Rarely requires treatment interruption.
Hair thinning (alopecia)
Common (~15%)Diffuse thinning usually resolves after completing the treatment course.
Infusion reactions
Uncommon (~4%)Mild reactions (flushing, headache, nausea) can usually be managed by slowing the infusion rate. Severe reactions are rare.
Inflammatory bowel disease exacerbation
RareTepezza is not contraindicated in inflammatory bowel disease, but it may cause an exacerbation of pre-existing IBD (Crohn's disease or ulcerative colitis). Patients with known IBD should be monitored, and any flare in symptoms reported promptly.
Why an Oculoplastic Surgeon for TED Care?
TED is a complex, multi-stage disease that requires monitoring and management across its entire natural history — from the active inflammatory phase treated with Tepezza, through the stable phase where surgical rehabilitation is performed. An ASOPRS fellowship-trained oculoplastic surgeon is uniquely positioned to provide this continuity:
- Complete orbital expertise
ASOPRS fellowship-trained surgeons measure proptosis, grade CAS, and interpret orbital imaging to track disease response to Tepezza over time.
- Surgical backup when needed
When Tepezza produces a plateau — or when disease is inactive — oculoplastic surgeons perform orbital decompression, strabismus surgery, and eyelid recession.
- Seamless continuity of care
Patients receive complete TED management from one subspecialist rather than being referred between multiple providers.
- Endocrinology co-management
TED is driven by underlying thyroid autoimmunity. Oculoplastic surgeons coordinate care with your endocrinologist and assist with prior authorization for Tepezza infusions.
Find an Oculoplastic Surgeon for TED
Use our directory to find an ASOPRS fellowship-trained oculoplastic surgeon in your area who specializes in Thyroid Eye Disease and Tepezza therapy.
Find a Doctor Near You →