Diagnosis and treatment of essential blepharospasm and hemifacial spasm — including botulinum toxin injection and surgical myectomy.
Medically reviewed by EyePlastics Medical Editorial Board·ASOPRS oculoplastic surgeons·Last updated June 2026
What is Blepharospasm
Blepharospasm refers to involuntary, forceful closure of the eyelids due to sustained or intermittent contraction of the orbicularis oculi muscle. It ranges from mild, occasional blinking to severely debilitating functional blindness from inability to open the eyes. Two distinct conditions are treated by oculoplastic surgeons: essential blepharospasm and hemifacial spasm.
Blepharospasm and hemifacial spasm are neurological conditions — initial evaluation often involves both neurology and oculoplastic surgery. Related conditions include Lagophthalmos (a separate problem of incomplete closure) and Eyelid Laxity.
Essential Blepharospasm
Essential blepharospasm (EB) is a focal dystonia — an involuntary movement disorder — characterized by bilateral, synchronous, sustained contraction of the orbicularis oculi. It begins subtly with increased blinking or mild lid spasm and can progress to near-complete functional blindness.
Symptoms
Increased blinking, particularly in bright light or when reading
Involuntary forced eyelid closure lasting seconds to minutes
Bilateral involvement (distinguishes EB from hemifacial spasm)
Exacerbated by fatigue, stress, and bright lighting
Temporarily relieved by sensory tricks — touching the face, talking, singing ("geste antagoniste")
Functionally disabling in moderate-to-severe cases: inability to drive, read, or work
▶ What Blepharospasm Looks Like
Patient education: a patient with benign essential blepharospasm — involuntary, forceful spasms of the eyelids. (This video shows the condition itself, not a treatment.)
Pathophysiology
Essential blepharospasm results from abnormal activity in the basal ganglia-thalamo-cortical circuitry, leading to excessive activation of the orbicularis oculi. It is not a primary eye condition but a central motor control disorder. Dry eye and ocular surface irritation can trigger or worsen spasm, which is why addressing ocular surface disease is part of comprehensive management.
Hemifacial Spasm
Hemifacial spasm (HFS) is a distinct condition caused by aberrant pulsatile compression of the facial nerve (CN VII) at its root exit zone from the brainstem, typically by a blood vessel (most commonly the anterior inferior cerebellar artery (AICA) or posterior inferior cerebellar artery (PICA)). This results in unilateral, involuntary contractions of the facial muscles.
Distinguishing Features
Unilateral — almost always involves only one side of the face (rare bilateral cases are usually asynchronous)
Begins with intermittent eyelid twitching, progressing to involve the lower face, cheek, and mouth
Not suppressible by sensory tricks
Contractions may persist during sleep (distinguishes HFS from psychogenic causes)
Long-standing HFS may cause mild facial weakness between spasms
Workup
MRI with gadolinium is recommended to evaluate the cerebellopontine angle and identify neurovascular compression. MRI also excludes mass lesions or demyelinating disease at the root exit zone.
Diagnosis
Clinical history and examination are central to diagnosis. The pattern (bilateral vs. unilateral), age of onset, progression, and associated neurological symptoms guide workup.
Electromyography (EMG) — can confirm synchronous discharge in multiple facial nerve branches characteristic of hemifacial spasm
MRI brain — evaluates for structural cause; mandatory in all HFS patients
Ocular surface evaluation — dry eye and trichiasis can trigger reflex blepharospasm and should be treated before attributing spasm to a dystonic cause
Botulinum Toxin (Botox) Treatment
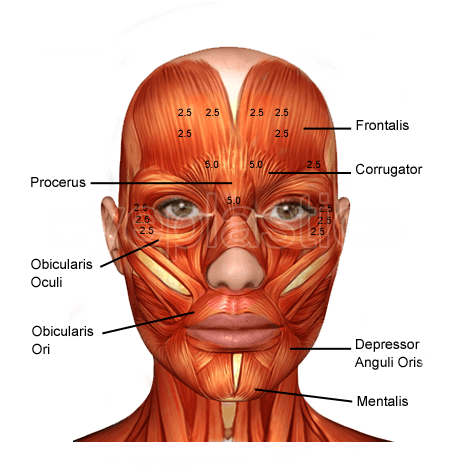
Injection technique — botulinum toxin placed into the orbicularis oculi
Botulinum toxin injection is the first-line treatment for both essential blepharospasm and hemifacial spasm. It is highly effective and generally well tolerated, with most patients obtaining meaningful symptom relief.
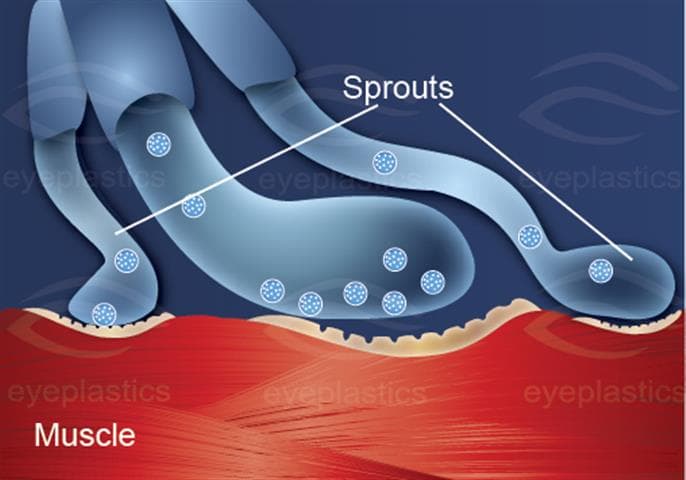
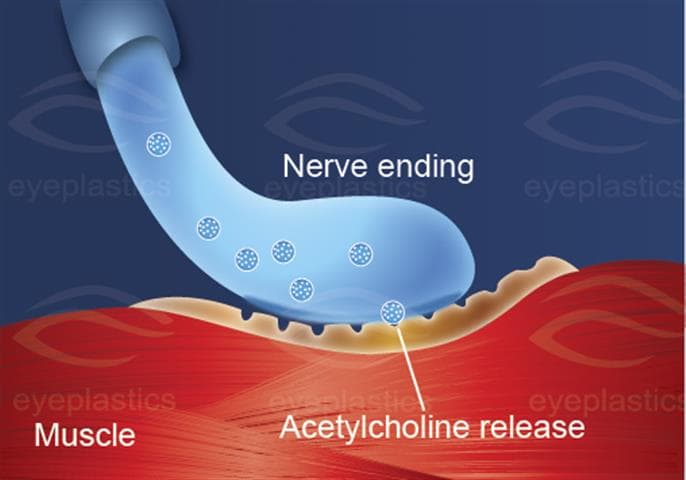
Mechanism
Botulinum toxin type A (onabotulinumtoxinA — Botox; abobotulinumtoxinA — Dysport; incobotulinumtoxinA — Xeomin) blocks acetylcholine release at the neuromuscular junction, producing a temporary, reversible chemical denervation of the injected muscle. For blepharospasm, small amounts are injected into the pretarsal and preseptal orbicularis oculi bilaterally.
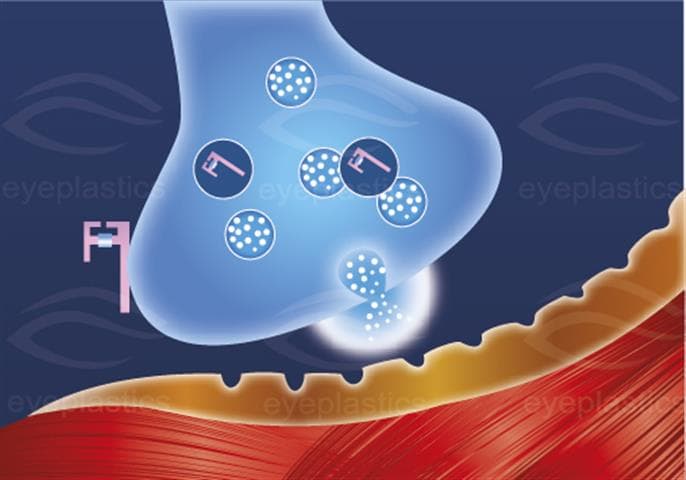
Mechanism of Action — Illustrated
Normal neuromuscular junctionSNARE complex — molecular targetAcetylcholine release blocked
Treatment Protocol
Orbicularis oculi — the primary muscle targeted in blepharospasm treatment
Injections performed in clinic under topical or no anesthesia using a fine needle
Effect begins in 2–4 days, reaches maximum at 7–14 days
Duration: approximately 3 months (8–16 weeks); retreatment every 3–4 months as needed
Most patients achieve excellent relief; response may diminish over years in some patients
Side Effects
Bruising at injection sites (common, temporary)
Ptosis — from diffusion to the levator; minimized with careful injection technique
Dry eye — from reduced blink rate after orbicularis weakening
Diplopia — rare; from diffusion to extraocular muscles
Surgical Myectomy
For patients with essential blepharospasm who have inadequate response to botulinum toxin, or who cannot tolerate injections, surgical myectomy is an option. The procedure involves excision of the orbicularis oculi, corrugator supercilii, and procerus muscles through upper and lower eyelid incisions.
Provides long-term relief in patients refractory to toxin injections
Upper eyelid approach allows removal of the pretarsal and preseptal orbicularis; lower lid and brow muscle excision through separate incisions
Risks include lagophthalmos, ectropion, scarring, and recurrence requiring repeat procedures
Most appropriate for severe, refractory essential blepharospasm
For hemifacial spasm refractory to botulinum toxin, microvascular decompression (MVD) — a neurosurgical procedure — is curative in 85–95% of cases when neurovascular compression is confirmed on MRI. This is performed by a neurosurgeon.
Support Groups & Resources
Blepharospasm is a chronic condition, and connecting with others who live with it makes a real difference. These organizations offer education, support communities, and research updates:
Essential blepharospasm is an involuntary, bilateral, sustained closure of the eyelids caused by abnormal neurological signals to the orbicularis oculi muscle. It is distinct from a normal eye twitch — patients cannot voluntarily open their eyes during a spasm, which significantly impairs daily function.
How is blepharospasm treated?
The first-line treatment is botulinum toxin (Botox, Dysport, or Xeomin) injected into the orbicularis oculi muscle, which provides 3–4 months of relief per treatment cycle. For patients who do not respond adequately to injections, surgical myectomy — removal of portions of the orbicularis muscle — provides longer-lasting relief.
Is blepharospasm the same as hemifacial spasm?
No. Blepharospasm is bilateral (both eyes) and starts in the eyelids. Hemifacial spasm is unilateral (one side of the face) and usually begins in the lower eyelid or cheek, caused by irritation of the facial nerve. Both are treated with botulinum toxin, but hemifacial spasm may also be cured by neurosurgical microvascular decompression.
How long do the results from botulinum toxin injections last?
Botulinum toxin injections typically provide relief from blepharospasm symptoms for 3 to 4 months, after which the effects gradually wear off. Most patients require repeat treatments 3 to 4 times per year to maintain symptom control. Some patients experience longer-lasting results over time as they receive repeated injections, while others may notice the duration varies slightly between treatments.
What should I expect during my consultation for blepharospasm treatment?
During your consultation, your oculoplastic surgeon will review your medical history, discuss when your symptoms began, and perform a thorough eye and facial examination. They will assess the severity of your spasms, discuss your treatment options (both nonsurgical and surgical), and explain what to expect with each approach. This is also an opportunity to ask questions about your specific condition and determine which treatment plan is right for you.
Am I a good candidate for surgical myectomy?
Candidates for surgical myectomy are typically patients who have had inadequate response to botulinum toxin injections or have developed resistance to the treatment. Your surgeon will evaluate factors such as the severity and pattern of your spasms, your overall health, and your personal preferences regarding treatment. Individuals who prefer a more permanent solution may also be good candidates after discussing the risks and benefits of surgery.
What is the recovery process like after blepharospasm surgery?
After surgical myectomy, most patients experience some swelling and bruising around the eyes for 1 to 2 weeks, during which time you should avoid strenuous activities. Your surgeon will provide specific post-operative instructions regarding eye care, activity restrictions, and when to resume normal routines. Most patients can return to light activities within a week and see full results within 4 to 6 weeks as swelling resolves and the muscles adjust.
Find a Specialist
Connect with a board-certified oculoplastic surgeon who specializes in blepharospasm.